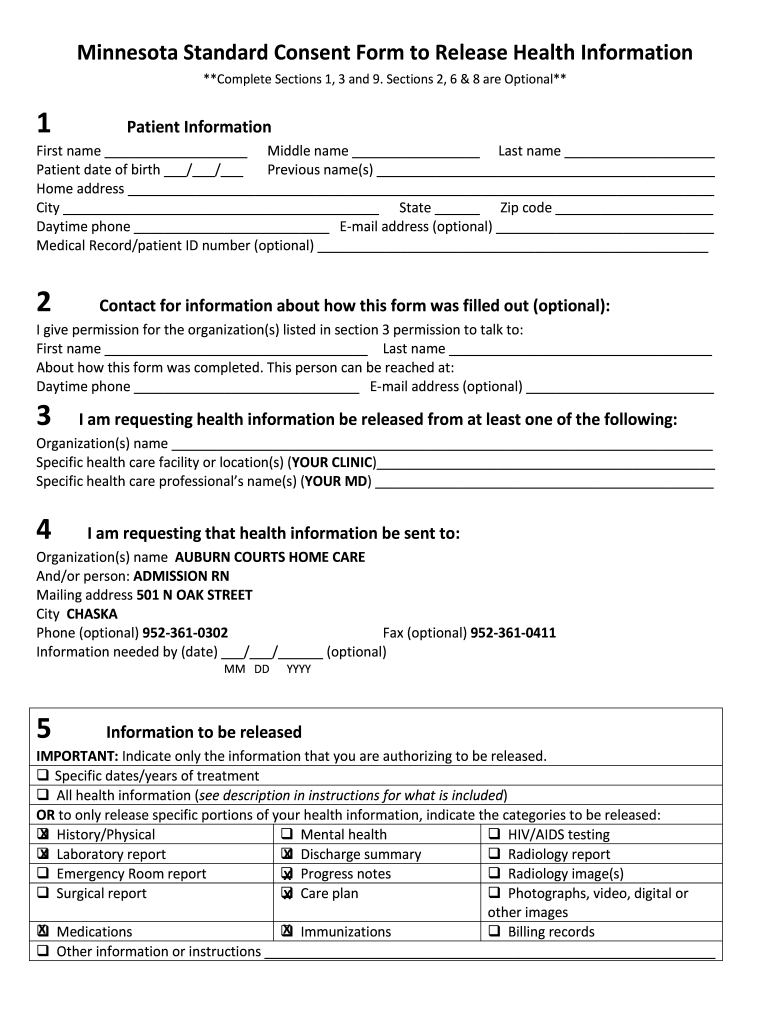
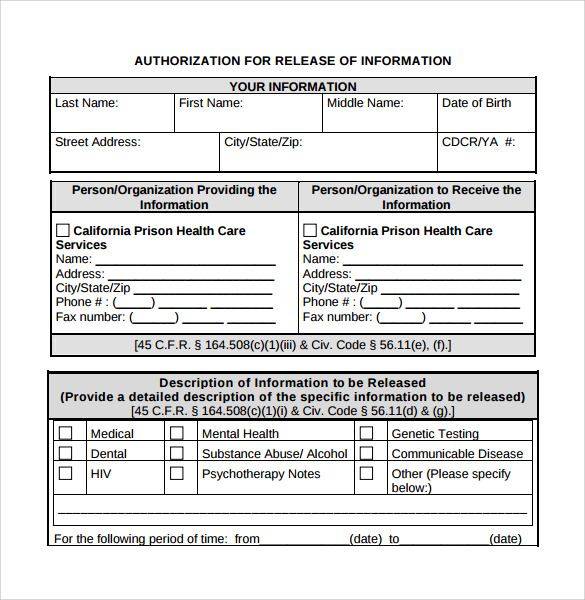
Release Of Information Form Mn - By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Have participants sign these forms if you are ever requesting or sharing private information. By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Instructions for minnesota standard consent form to release health information. Please read all instructions and information before completing. Voluntary authorization for release of medical and insurance information i, _____, date of birth: _____, authorize (print full name). Federal consent requirements to release health records were considered such as hipaa 45 cfr section 164.508, 42 cfr and minnesota statutes.
By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. _____, authorize (print full name). Instructions for minnesota standard consent form to release health information. By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Federal consent requirements to release health records were considered such as hipaa 45 cfr section 164.508, 42 cfr and minnesota statutes. Voluntary authorization for release of medical and insurance information i, _____, date of birth: Please read all instructions and information before completing. Have participants sign these forms if you are ever requesting or sharing private information.
Instructions for minnesota standard consent form to release health information. By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Voluntary authorization for release of medical and insurance information i, _____, date of birth: By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Please read all instructions and information before completing. Have participants sign these forms if you are ever requesting or sharing private information. Federal consent requirements to release health records were considered such as hipaa 45 cfr section 164.508, 42 cfr and minnesota statutes. _____, authorize (print full name).

Release Of Information Forms Printable (BLANK TEMPLATE)
By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. _____, authorize (print full name). Voluntary authorization for release of medical and insurance information i, _____, date of birth: Please read all instructions and information before completing. Federal consent requirements.
Release of information form mn Fill out & sign online DocHub
Have participants sign these forms if you are ever requesting or sharing private information. Voluntary authorization for release of medical and insurance information i, _____, date of birth: By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Please read.
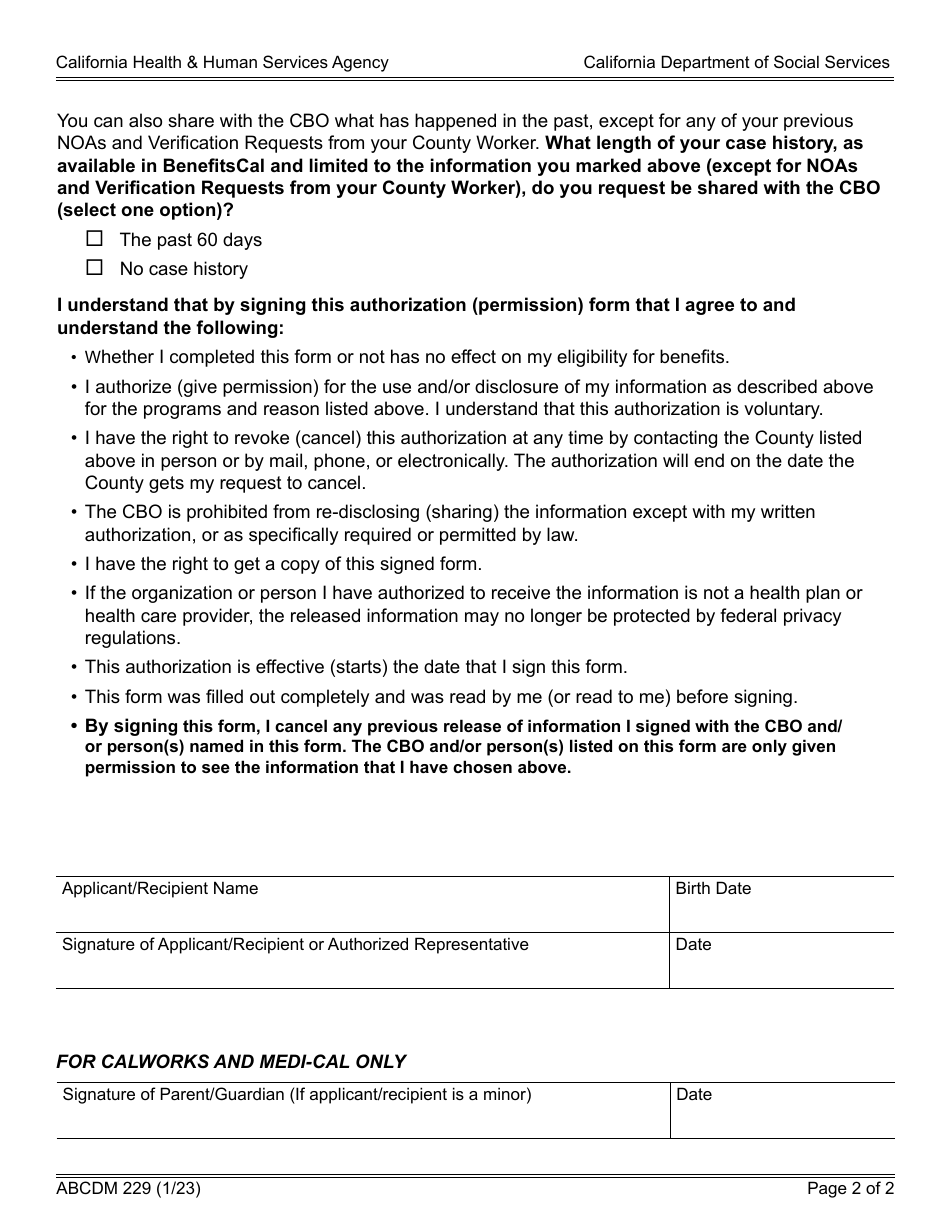
Form ABCDM229 Fill Out, Sign Online and Download Fillable PDF
Instructions for minnesota standard consent form to release health information. _____, authorize (print full name). By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. By indicating any of the categories in section 5, you are giving permission for written.
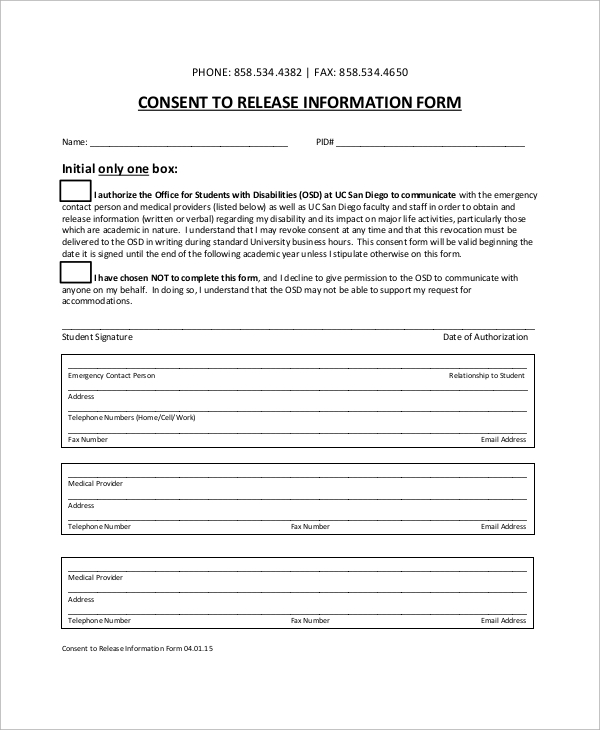
Information Release Form Template
Federal consent requirements to release health records were considered such as hipaa 45 cfr section 164.508, 42 cfr and minnesota statutes. Please read all instructions and information before completing. _____, authorize (print full name). Have participants sign these forms if you are ever requesting or sharing private information. Instructions for minnesota standard consent form to release health information.
Release Of Information Form Template
_____, authorize (print full name). Voluntary authorization for release of medical and insurance information i, _____, date of birth: Have participants sign these forms if you are ever requesting or sharing private information. Instructions for minnesota standard consent form to release health information. Federal consent requirements to release health records were considered such as hipaa 45 cfr section 164.508, 42.
9 Release Of Information Form Download for Free Sample Templates
Please read all instructions and information before completing. By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Voluntary authorization for release of medical and insurance information i, _____, date of birth: Instructions for minnesota standard consent form to release.

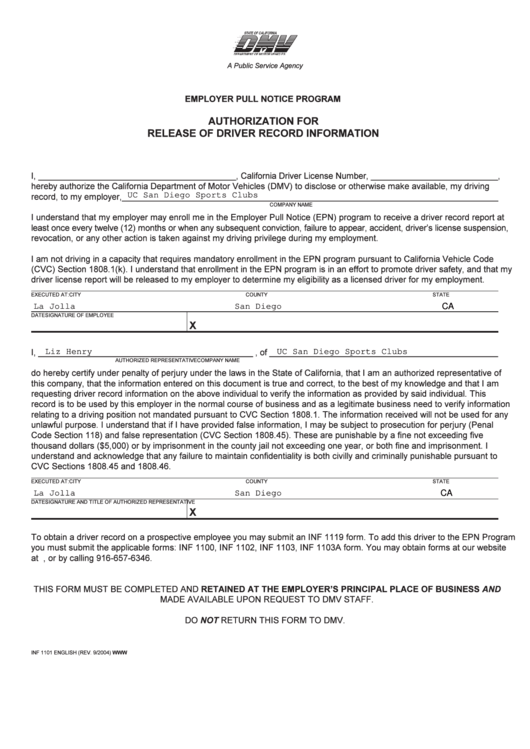
Employee Release Of Information Form MPLOYME
Federal consent requirements to release health records were considered such as hipaa 45 cfr section 164.508, 42 cfr and minnesota statutes. Please read all instructions and information before completing. Voluntary authorization for release of medical and insurance information i, _____, date of birth: By indicating any of the categories in section 5, you are giving permission for written information to.
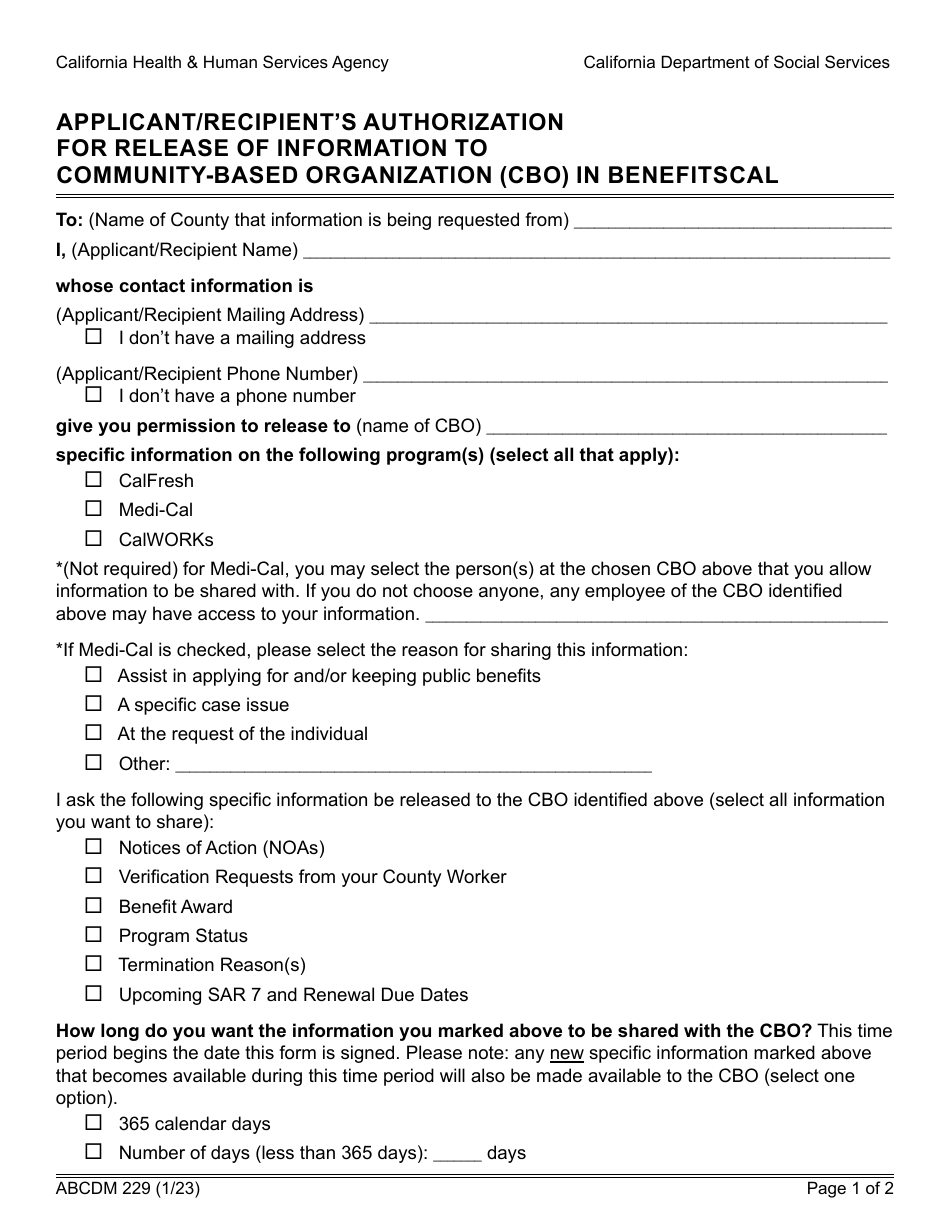
Form ABCDM229 Fill Out, Sign Online and Download Fillable PDF
Have participants sign these forms if you are ever requesting or sharing private information. Voluntary authorization for release of medical and insurance information i, _____, date of birth: By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. By indicating.

Information Release Form Template
By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Please read all instructions and information before completing. By indicating any of the categories in section 5, you are giving permission for written information to be released and for a.
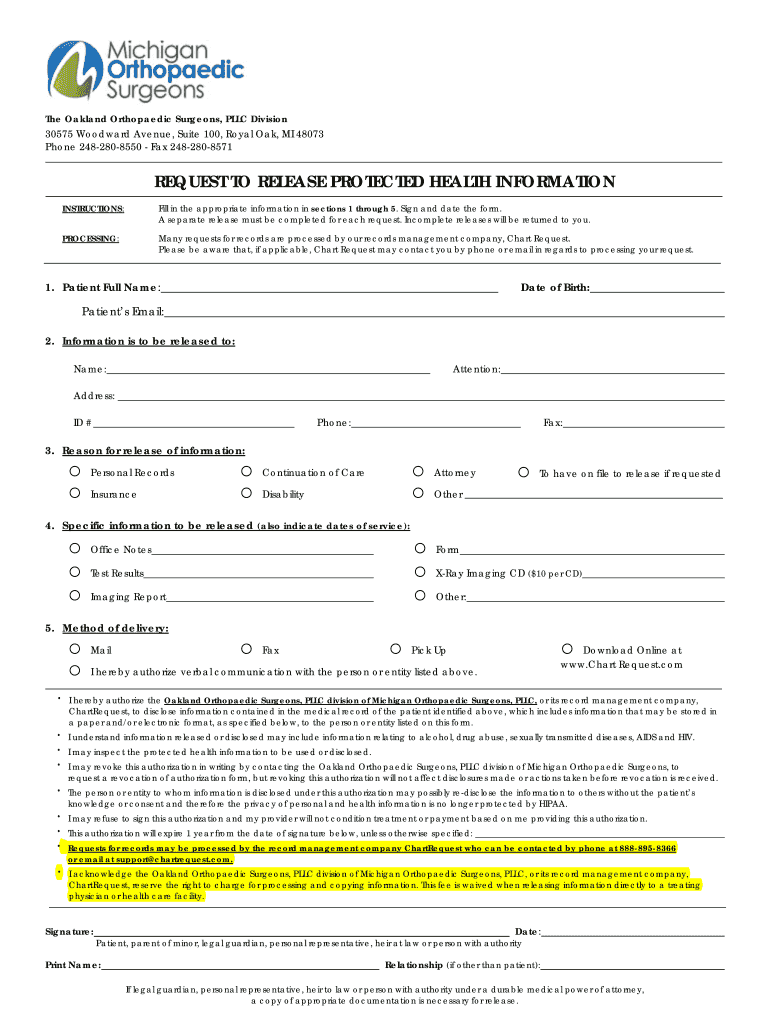
Request to Release Protected Health Information Form MOS 02 Fill Out
Voluntary authorization for release of medical and insurance information i, _____, date of birth: By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Instructions for minnesota standard consent form to release health information. Have participants sign these forms if.
Instructions For Minnesota Standard Consent Form To Release Health Information.
Please read all instructions and information before completing. By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Federal consent requirements to release health records were considered such as hipaa 45 cfr section 164.508, 42 cfr and minnesota statutes. Have participants sign these forms if you are ever requesting or sharing private information.
_____, Authorize (Print Full Name).
By indicating any of the categories in section 5, you are giving permission for written information to be released and for a person in section 3 to talk to a. Voluntary authorization for release of medical and insurance information i, _____, date of birth: