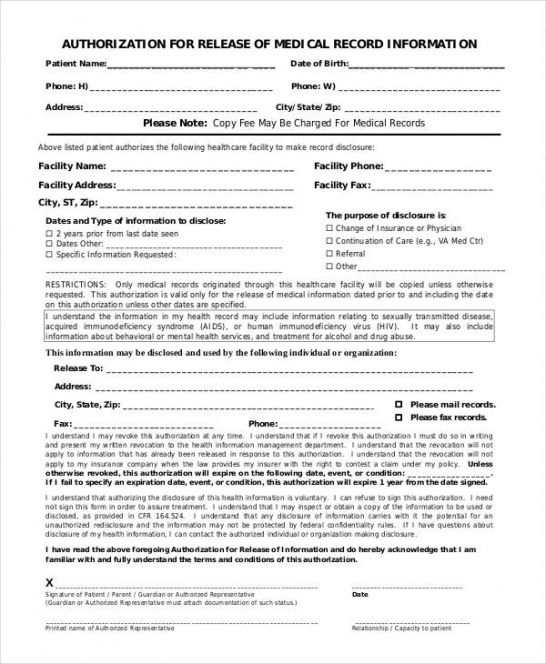
Release Of Information Form In Spanish - Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: 4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. ⚫ tengo el derecho de negarme a firmar este. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0.
Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. 4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. ⚫ tengo el derecho de negarme a firmar este.
4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. ⚫ tengo el derecho de negarme a firmar este.
Top Release Form In Spanish Templates free to download in PDF format
960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. ⚫ tengo el derecho de negarme a firmar este. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. This form is to be used by a patient or legal representative to authorize the release of information to a third party.
Free Authorization To Release Medical Records Form Template Word
La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. 4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para..

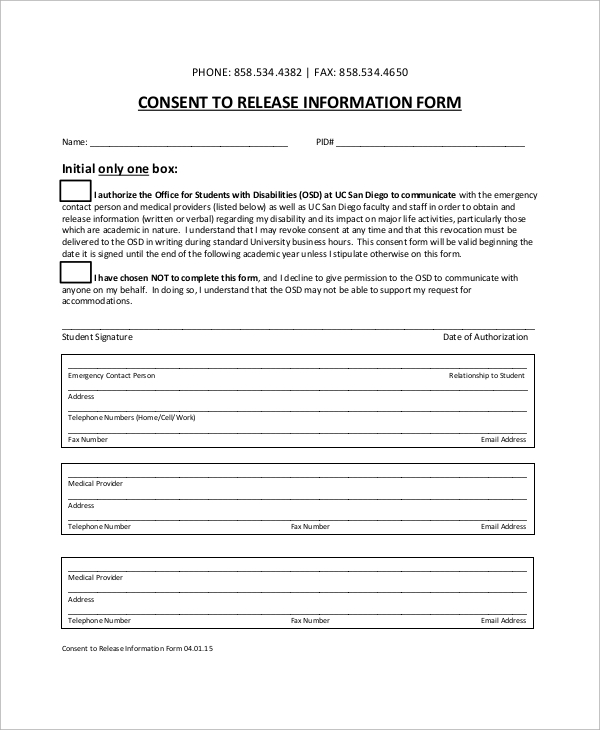
Printable Spanish Patient Registration Form Printable Forms Free Online
4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. ⚫ tengo el.
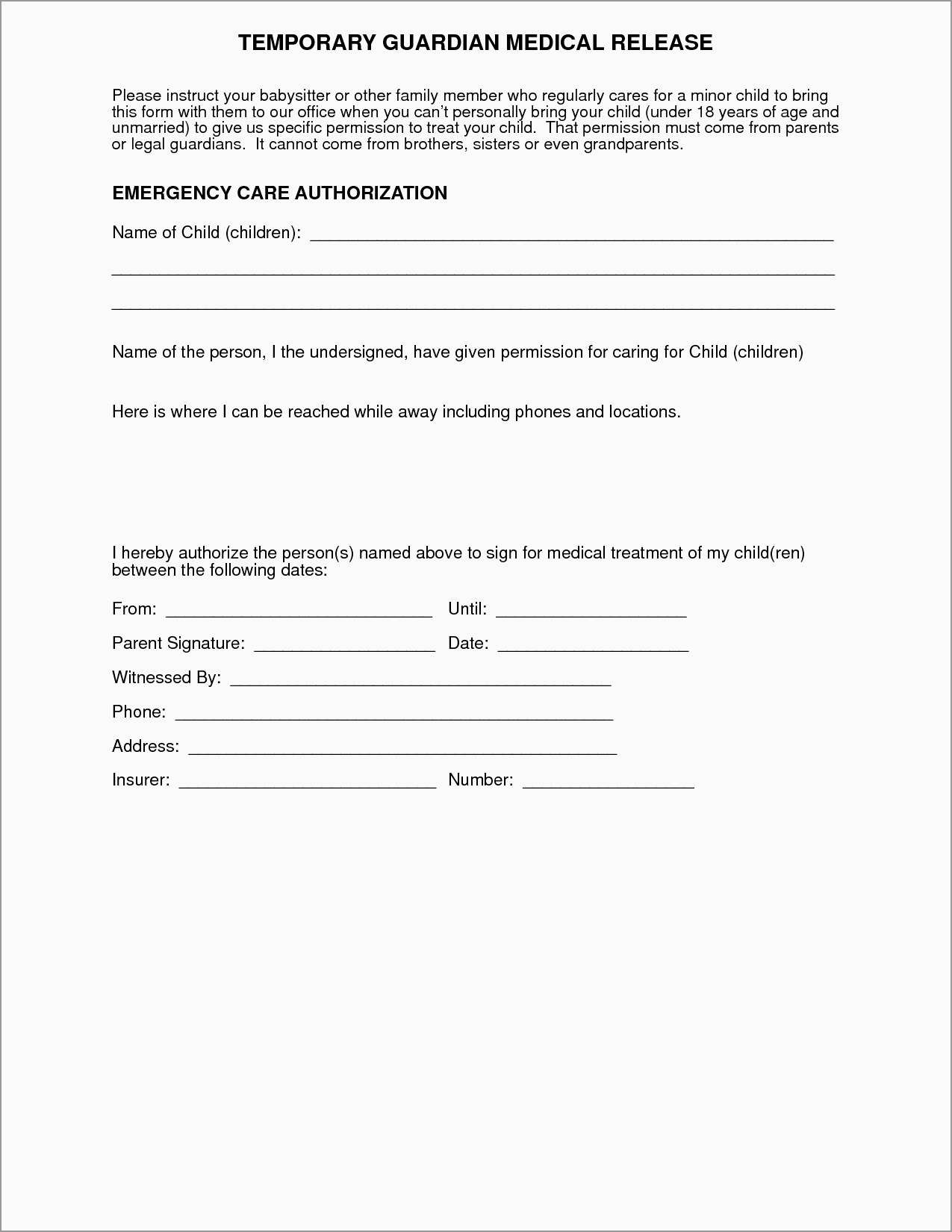
Free Printable Medical Consent Form For Trainers Printable Forms Free
Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: ⚫ tengo el derecho de negarme a firmar.
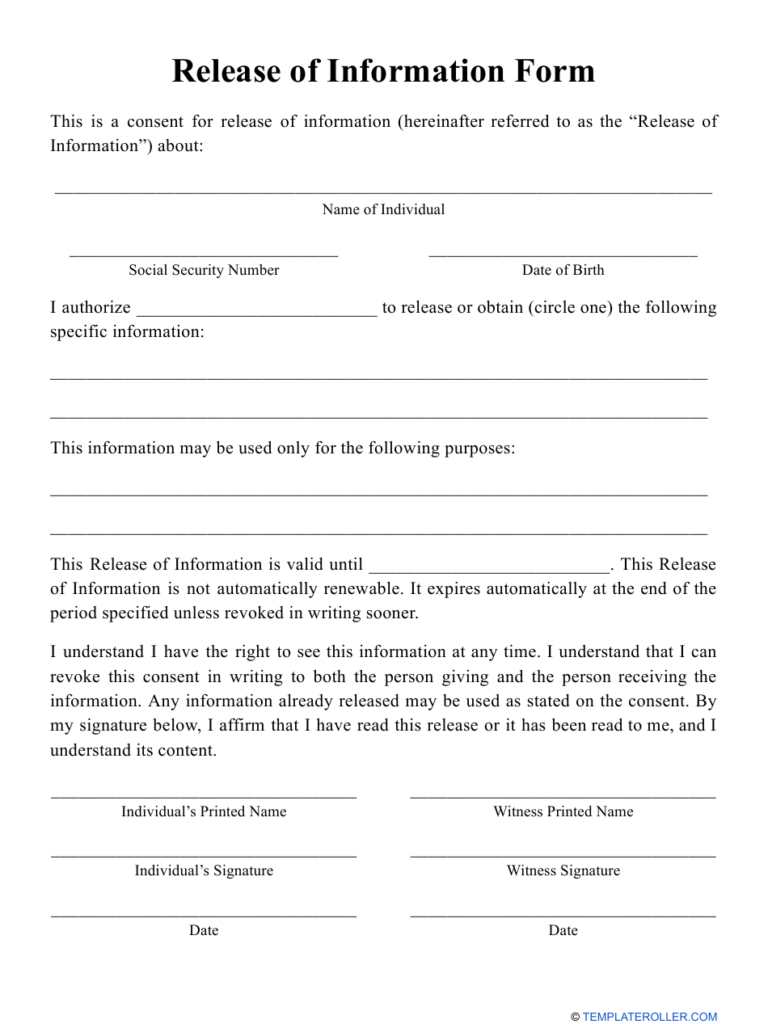
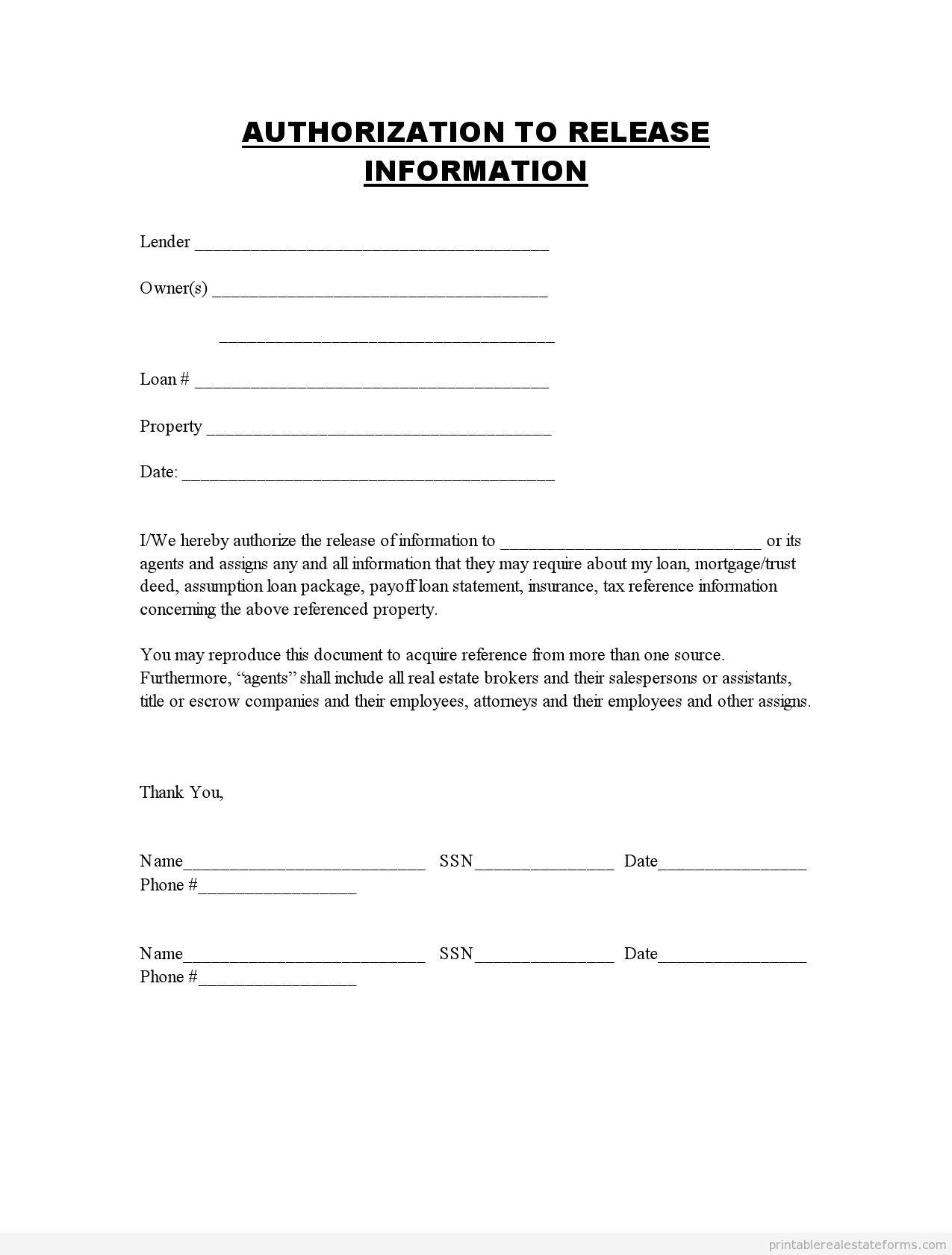
Release Of Information Form Download Printable PDF Templateroller
Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. This form is to be used by a patient or legal representative to authorize the release of information to a third.
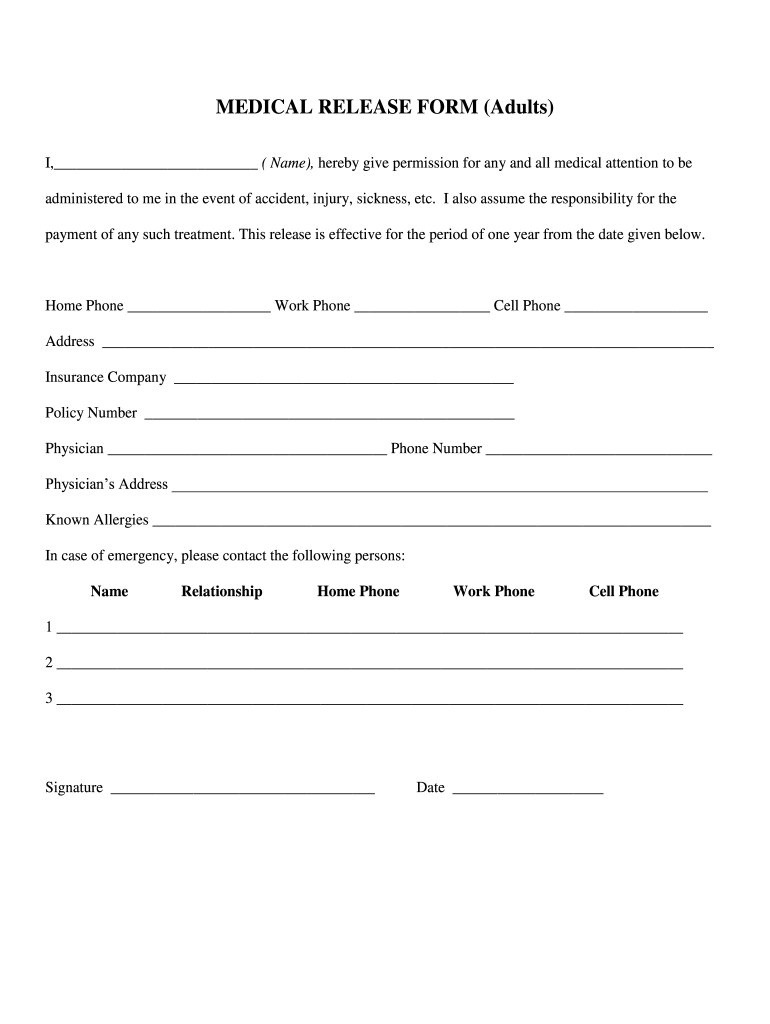
Medical Release Form 20202022 Fill and Sign Printable Template
960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. ⚫ tengo el derecho de negarme a firmar este. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: 4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. Authorization for release of.
Consent Release Of Information Authorization Form
Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. 4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. ⚫ tengo el.
Information Release Form Template
This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization to use, disclose & release protected health information (spanish) entiendo.
Medical Release Form Printable
4/2024 coloque la etiqueta del paciente aquí (solo para uso interno) *si se trata de comunicación oral, complete la autorización para. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other.

HIPAA Authorisation Form YouTube
960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente: This form is to be used by a patient or legal.
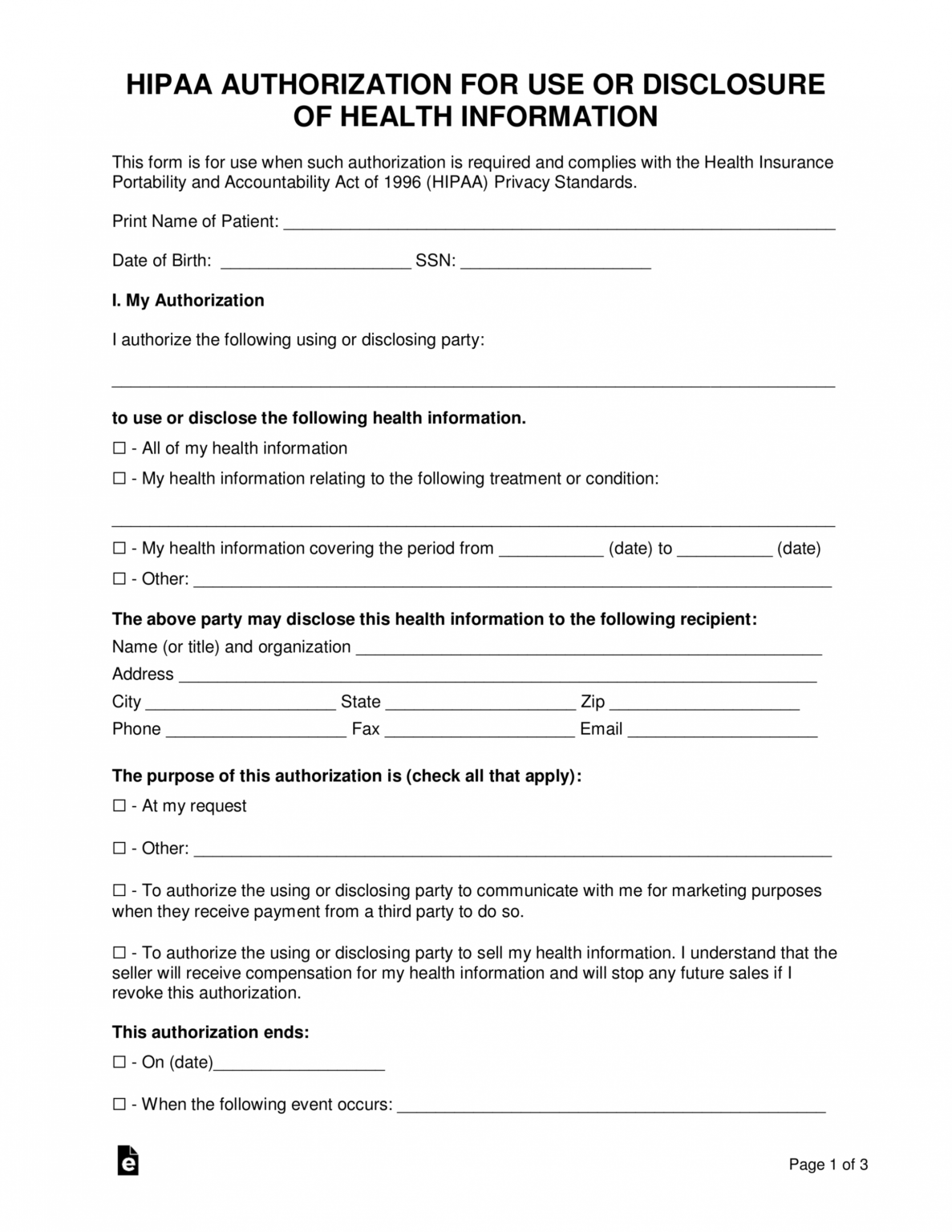
This Form Is To Be Used By A Patient Or Legal Representative To Authorize The Release Of Information To A Third Party (Other Than A Family.
La información indicada anteriormente se puede divulgar a / (physician / clinic or practice name to release your records) may release the above. Authorization for release of health information (spanish) authorization for release of health information (spanish) 5 0. 960 autorización para divulgar información médica de conformidad con hipaa [este formulario fue. Authorization to use, disclose & release protected health information (spanish) entiendo lo siguiente:
4/2024 Coloque La Etiqueta Del Paciente Aquí (Solo Para Uso Interno) *Si Se Trata De Comunicación Oral, Complete La Autorización Para.
⚫ tengo el derecho de negarme a firmar este.