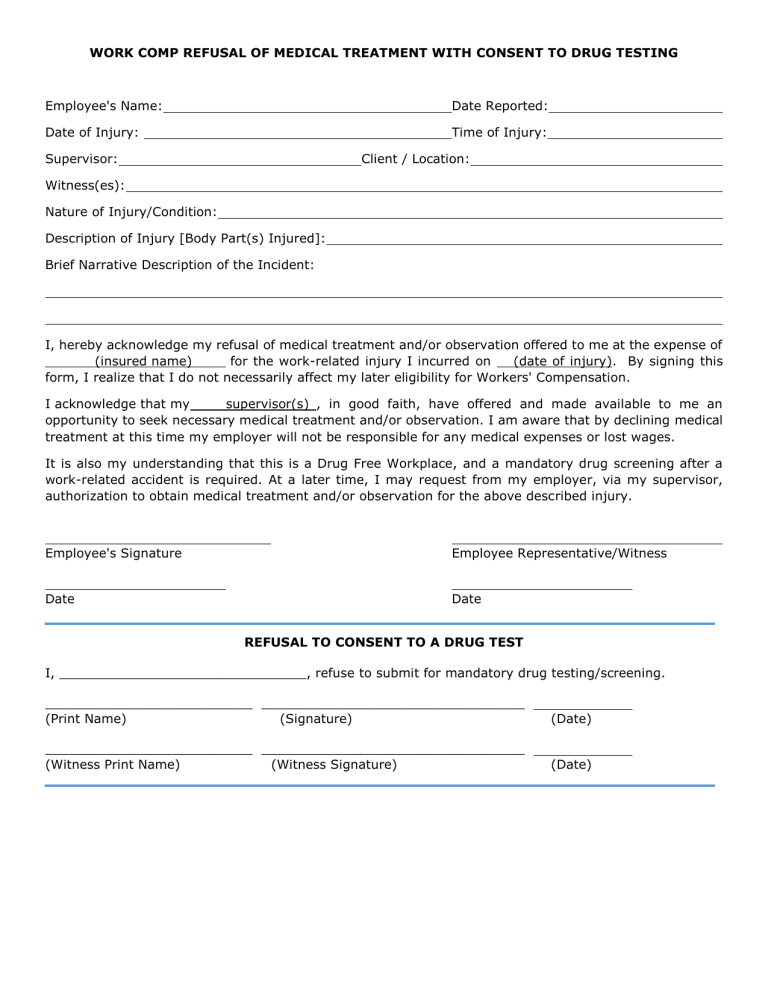
Refuse Medical Treatment Form - I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Use this form if an employee has a minor injury and they do not feel that they need medical treatment. If the employee’s injury is obvious, get medical. Medical treatment has been offered to me;.
I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. Use this form if an employee has a minor injury and they do not feel that they need medical treatment. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Medical treatment has been offered to me;. If the employee’s injury is obvious, get medical. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.:
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: Use this form if an employee has a minor injury and they do not feel that they need medical treatment. If the employee’s injury is obvious, get medical. Medical treatment has been offered to me;. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________.

Medical Treatment Refusal Form Template amulette
I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. Medical treatment has been offered to me;. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. By signing below, i understand that my refusal to follow my providers advice.
FREE 43+ Printable Medical Forms in PDF
Use this form if an employee has a minor injury and they do not feel that they need medical treatment. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended.
Against medical advice form Fill out & sign online DocHub
If the employee’s injury is obvious, get medical. Medical treatment has been offered to me;. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness.
Fillable Refusal Of Treatment Form printable pdf download
I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. If the employee’s injury is obvious, get medical. Use this form if an employee has a minor injury and they do not feel that they need medical treatment. My signature below confirms that i am not experiencing any signs.
Medical Treatment Refusal Form Template Amulette
Use this form if an employee has a minor injury and they do not feel that they need medical treatment. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________..

Is it a sin to refuse medical treatment?
I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Medical treatment has been offered to me;. I, hereby acknowledge my declination of medical treatment.

Refusal of Treatment Certificate Competent Person
Medical treatment has been offered to me;. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. I, hereby acknowledge my declination of medical.
Refusal of Medical Treatment or Observation
I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. Medical treatment has been offered to me;. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. My signature below confirms that.

Do I have the right to refuse medical treatment? YouTube
Medical treatment has been offered to me;. I, _____, refuse to consent to the following treatment/procedure/ diagnostic test/medication/referral as recommended by my physician, _______________ m.d./d.o.: By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. I, hereby acknowledge my declination of medical treatment.

Refusal of Dental Treatment Form PDF airSlate SignNow
Use this form if an employee has a minor injury and they do not feel that they need medical treatment. If the employee’s injury is obvious, get medical. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Medical treatment has been offered.
If The Employee’s Injury Is Obvious, Get Medical.
I, hereby acknowledge my declination of medical treatment and/or observation offered to me by_______________________for the injury or illness reported on ______________________. My signature below confirms that i am not experiencing any signs or symptoms resulting from the incident/accident described above. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could seriously impair my health or even result in. Use this form if an employee has a minor injury and they do not feel that they need medical treatment.
I, _____, Refuse To Consent To The Following Treatment/Procedure/ Diagnostic Test/Medication/Referral As Recommended By My Physician, _______________ M.d./D.o.:
Medical treatment has been offered to me;.