Geisinger Medical Records Release Form - I authorize an appropriate workforce member of the above entity(ies) to release information from my medical record to: Release of information marworth geisinger health system1 patient name: Patients who have received care at this facility may request copies of their medical records/health information to be released to. You can submit a medical release to:. Health information management release of medical information 100 n. To request release of medical information please complete and sign this form i, ____________________________________hereby. I am requesting records from the following geisinger entities: Luke’s university health network, medical records department, 77 commerce way, bethlehem, pa 18017. I authorize an appropriate workforce member of the. All sites specific clinic(s) or hospital(s):
I authorize an appropriate workforce member of the above entity(ies) to release information from my medical record to: Fax or mail the form to geisinger at: Health information management release of medical information 100 n. All sites specific clinic(s) or hospital(s): Patients who have received care at this facility may request copies of their medical records/health information to be released to. I authorize an appropriate workforce member of the. To request release of medical information please complete and sign this form i, ____________________________________hereby. You can submit a medical release to:. (name of hospital, company or. Complete and sign the form ;
I authorize an appropriate workforce member of the. Complete and sign the form ; (name of hospital, company or. Luke’s university health network, medical records department, 77 commerce way, bethlehem, pa 18017. Release of information marworth geisinger health system1 patient name: I am requesting records from the following geisinger entities: You can submit a medical release to:. Fax or mail the form to geisinger at: I authorize an appropriate workforce member of the above entity(ies) to release information from my medical record to: All sites specific clinic(s) or hospital(s):

Fillable Online Healthy Rewards Reimbursement Request Form for
(name of hospital, company or. I authorize an appropriate workforce member of the above entity(ies) to release information from my medical record to: All sites specific clinic(s) or hospital(s): I am requesting records from the following geisinger entities: Complete and sign the form ;

News Release Geisinger Wyoming Valley Medical Center cuts ribbon on
Release of information marworth geisinger health system1 patient name: All sites specific clinic(s) or hospital(s): I am requesting records from the following geisinger entities: You can submit a medical release to:. Fax or mail the form to geisinger at:
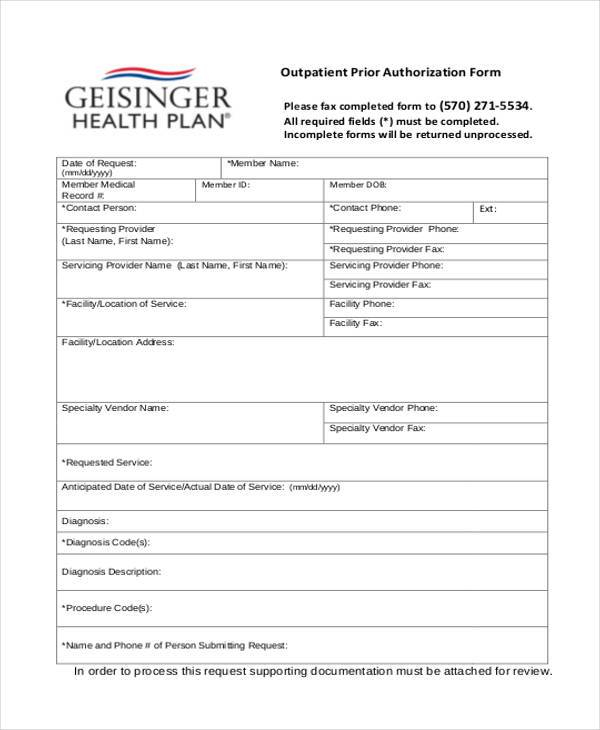
Completing The GHP Prior Authorization Request Form Geisinger
Health information management release of medical information 100 n. I am requesting records from the following geisinger entities: (name of hospital, company or. To request release of medical information please complete and sign this form i, ____________________________________hereby. All sites specific clinic(s) or hospital(s):
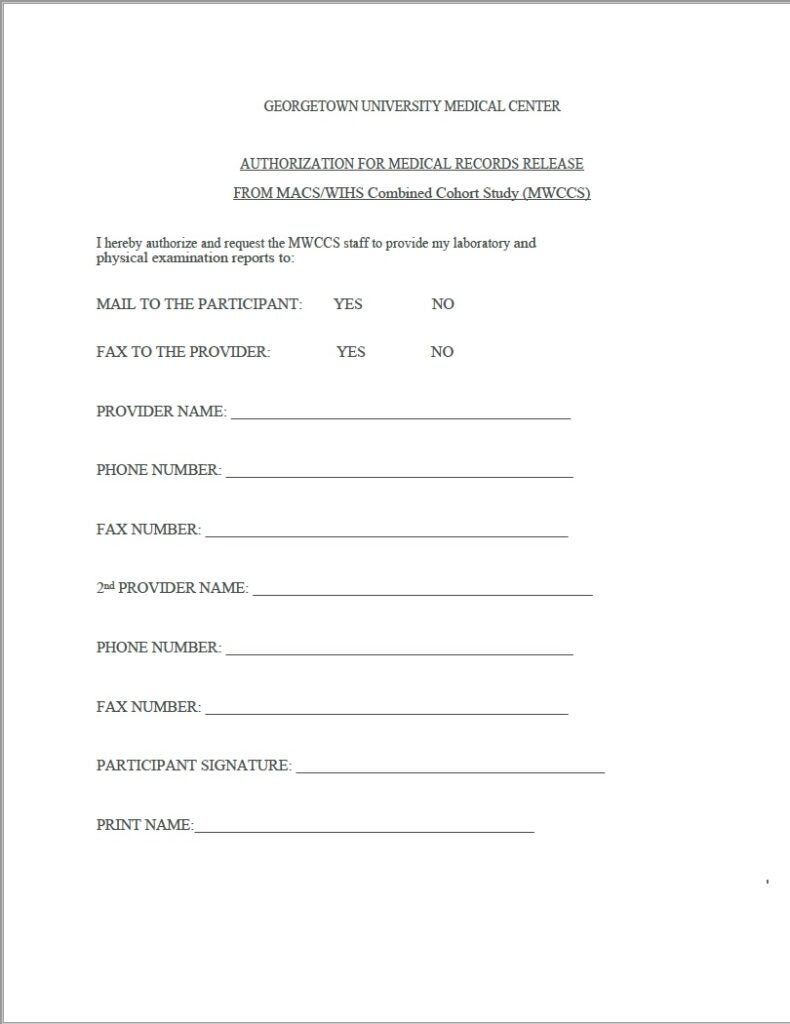
FAQ DC MWCCS & STAR University
Luke’s university health network, medical records department, 77 commerce way, bethlehem, pa 18017. I authorize an appropriate workforce member of the. I authorize an appropriate workforce member of the above entity(ies) to release information from my medical record to: (name of hospital, company or. I am requesting records from the following geisinger entities:

Free Medical Records Release Form (HIPAA) PDF Word
Luke’s university health network, medical records department, 77 commerce way, bethlehem, pa 18017. You can submit a medical release to:. Fax or mail the form to geisinger at: Complete and sign the form ; I am requesting records from the following geisinger entities:

Best Authorization To Release Medical Records Guide 2024 Guide
I authorize an appropriate workforce member of the. You can submit a medical release to:. I authorize an appropriate workforce member of the above entity(ies) to release information from my medical record to: Complete and sign the form ; I am requesting records from the following geisinger entities:

Fillable Online HIPAA & Geisinger Release Form Fax Email Print pdfFiller
I authorize an appropriate workforce member of the above entity(ies) to release information from my medical record to: Complete and sign the form ; Health information management release of medical information 100 n. I am requesting records from the following geisinger entities: You can submit a medical release to:.
Geisinger study of blood test for cancer shows promising results
Luke’s university health network, medical records department, 77 commerce way, bethlehem, pa 18017. I authorize an appropriate workforce member of the. Health information management release of medical information 100 n. I am requesting records from the following geisinger entities: Patients who have received care at this facility may request copies of their medical records/health information to be released to.

Massachusetts Medical Records Release Form Download Free Printable
Fax or mail the form to geisinger at: I authorize an appropriate workforce member of the. You can submit a medical release to:. I authorize an appropriate workforce member of the above entity(ies) to release information from my medical record to: Complete and sign the form ;

Fillable Online McLean Hospital Medical Records Release Form Fax Email
To request release of medical information please complete and sign this form i, ____________________________________hereby. All sites specific clinic(s) or hospital(s): Complete and sign the form ; Luke’s university health network, medical records department, 77 commerce way, bethlehem, pa 18017. You can submit a medical release to:.
I Authorize An Appropriate Workforce Member Of The Above Entity(Ies) To Release Information From My Medical Record To:
Complete and sign the form ; To request release of medical information please complete and sign this form i, ____________________________________hereby. Luke’s university health network, medical records department, 77 commerce way, bethlehem, pa 18017. Release of information marworth geisinger health system1 patient name:
Fax Or Mail The Form To Geisinger At:
I am requesting records from the following geisinger entities: You can submit a medical release to:. Health information management release of medical information 100 n. Patients who have received care at this facility may request copies of their medical records/health information to be released to.
(Name Of Hospital, Company Or.
I authorize an appropriate workforce member of the. All sites specific clinic(s) or hospital(s):