Broadreach Medical Resources Prior Authorization Form - By signing this form i authorize broadreach medical resources, inc. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser. This medical form is due 60 days prior to your program start date. Attach copies of prescription receipt showing: Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. Hereafter “bmr” and the service providers for my selected plan to send. If you are unable to return this completed form on time, we prefer to receive an.
By signing this form i authorize broadreach medical resources, inc. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. If you are unable to return this completed form on time, we prefer to receive an. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser. Hereafter “bmr” and the service providers for my selected plan to send. Attach copies of prescription receipt showing: This medical form is due 60 days prior to your program start date.
Attach copies of prescription receipt showing: By signing this form i authorize broadreach medical resources, inc. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. This medical form is due 60 days prior to your program start date. Hereafter “bmr” and the service providers for my selected plan to send. If you are unable to return this completed form on time, we prefer to receive an. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser.

Kroger Prescription Plan Prior Authorization Form
This medical form is due 60 days prior to your program start date. Hereafter “bmr” and the service providers for my selected plan to send. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. By signing this form i authorize broadreach medical resources, inc. All eligible active employees and retired participants enrolled in the indemnity.
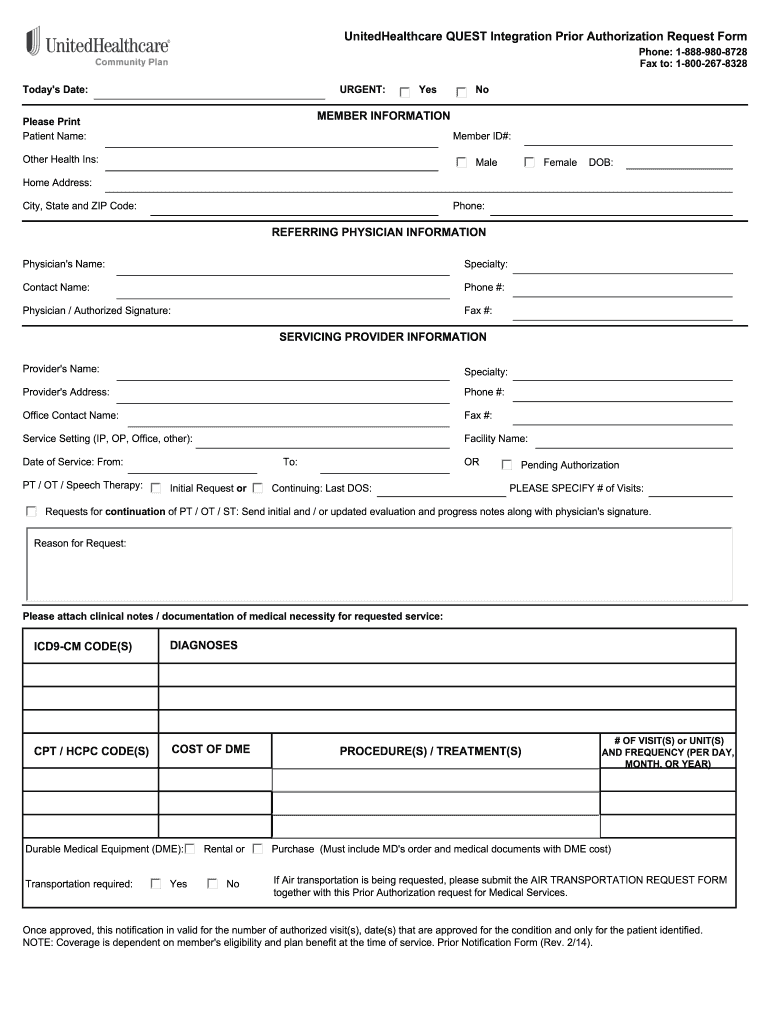
United Healthcare Prior Authorization Forms Fill Online, Printable
By signing this form i authorize broadreach medical resources, inc. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. This medical form is due 60 days prior to your program start date. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser. If you are.

Broadreach Medical Resources SQFactory
Attach copies of prescription receipt showing: By signing this form i authorize broadreach medical resources, inc. If you are unable to return this completed form on time, we prefer to receive an. This medical form is due 60 days prior to your program start date. Hereafter “bmr” and the service providers for my selected plan to send.
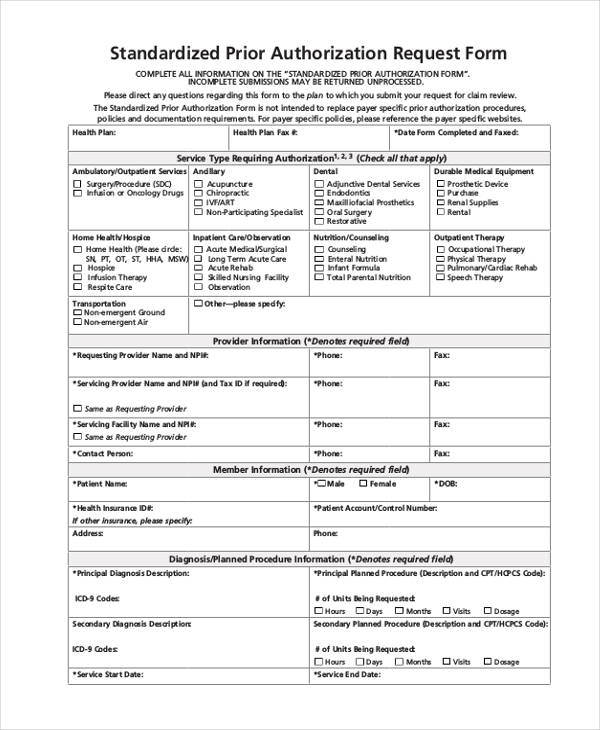
FREE 13+ Prior Authorization Forms in PDF MS Word
Hereafter “bmr” and the service providers for my selected plan to send. This medical form is due 60 days prior to your program start date. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. If.
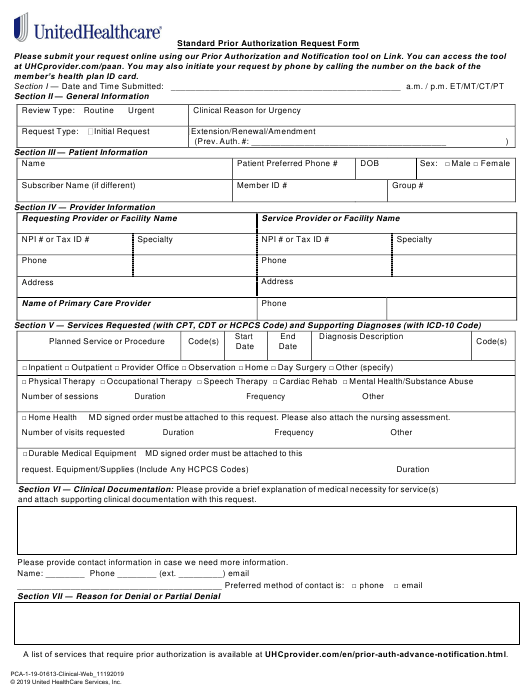
Unitedhealthcare Community Plan Prior Authorization Form Washington
All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. This medical form is due 60 days prior to your program start date. If you are unable to return this completed form on time, we prefer.

Healthfirst Leaf Plans Prior Authorization Forms
By signing this form i authorize broadreach medical resources, inc. Attach copies of prescription receipt showing: Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. This medical form is due 60 days prior to your program start date. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for.
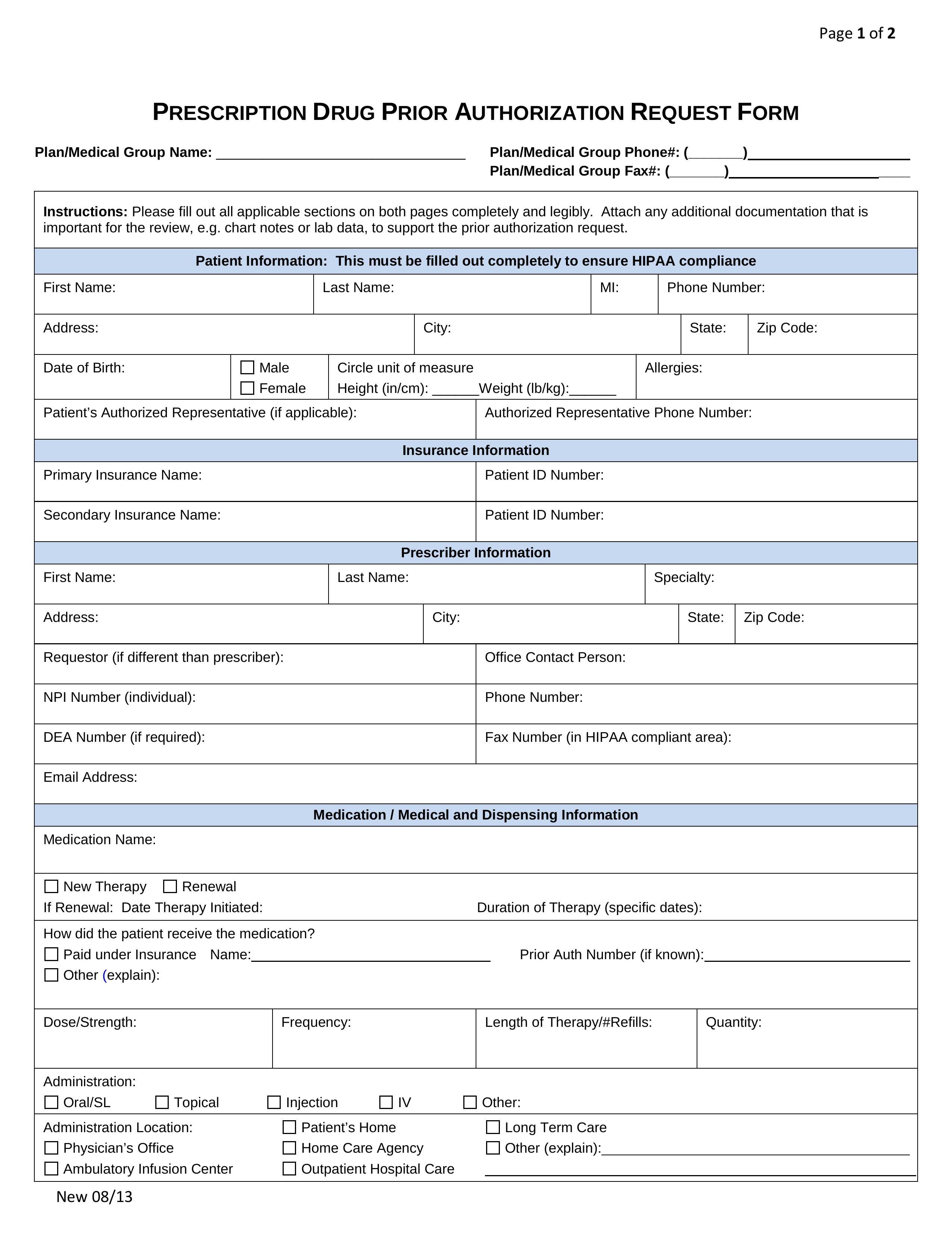
Free Prior (Rx) Authorization Forms PDF eForms
Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. This medical form is due 60 days prior to your program start date. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser. Attach copies of prescription receipt showing: By signing this form i authorize broadreach.

Electronic Prior Authorization Medication Access Report CoverMyMeds
Attach copies of prescription receipt showing: Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser. By signing this form i authorize broadreach medical resources, inc. This medical form is due 60 days prior to your.

Working at BMR Great Place To Work®
If you are unable to return this completed form on time, we prefer to receive an. Hereafter “bmr” and the service providers for my selected plan to send. Attach copies of prescription receipt showing: This medical form is due 60 days prior to your program start date. All eligible active employees and retired participants enrolled in the indemnity medical and.
Fillable Online Broadreach Medical Resources, Inc Fax Email Print
If you are unable to return this completed form on time, we prefer to receive an. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser. By signing this form i authorize broadreach medical resources, inc. Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity..
Hereafter “Bmr” And The Service Providers For My Selected Plan To Send.
Pharmacy name, prescription number, drug name, drug cost, patient name, fill date and quantity. If you are unable to return this completed form on time, we prefer to receive an. By signing this form i authorize broadreach medical resources, inc. All eligible active employees and retired participants enrolled in the indemnity medical and hmo programs (except for members of kaiser.
Attach Copies Of Prescription Receipt Showing:
This medical form is due 60 days prior to your program start date.